


Content warning: Suicide
I
There is a lot of suffering in the world, as r/depression can remind you. Every day in every town, there are people who do not want to live anymore. The existential pain and psychological torment they experience are overbearing. Fortunately, despite all the stigma surrounding mental health, they typically seek help when they hit these low points. Hence, the well-acknowledged fact in the healthcare field that the majority of people who die by suicide visit a healthcare provider in the few months prior to their death. The words ‘I don’t want to live’ and any of its varieties are a red flag for any healthcare providers, and their utterance results in being whisked away to the emergency department.
What does help at the ED look like? After arriving to the emergency department, you’ll probably wait in a waiting room (or on a bed in a hallway) for a few hours until a mental health professional (social worker, psychiatrist, etc.) meets with you to explore what’s been going on and discuss how the you’ve been feeling. Their primary goal during this conversation is deciding - do I place this person on a legal ‘danger to self’ hold and force them into an inpatient hospitalization in order to keep them safe, or discharge them home with close follow-up and extra support.
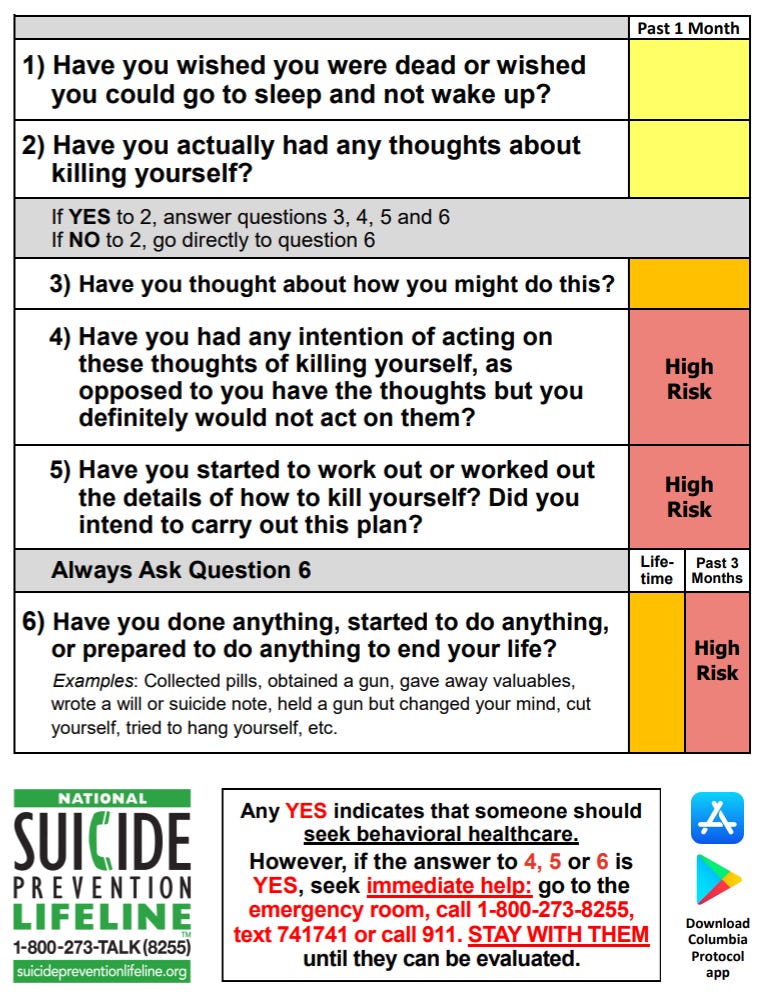
The answer to this question is not always apparent. When someone says they don’t want to live anymore - does that mean they want to kill themselves? When someone says they want to kill themselves - does that mean they actually want to kill themselves? Does cutting oneself superficially to feel something other than emptiness correlate with taking one’s life? How emotionally stable is the person - are they fine one minute and suicidal the next? Are drugs involved? Are they a SAD PERSON? These types of questions and more are being considered in the risk assessment, and clinicians have data and clinical experience to help stratify how much risk this person is at for completing suicide.
There is an asymmetry in the severity of consequences with this decision. Sending someone to inpatient hospitalization when they didn’t need it seems a much better outcome than not admitting someone who needed it and proceeds to die by suicide. In other words, a Type 1 error (false positive - patient deemed to about to commit suicide, but in actuality was not going to) is generally thought of as better than a type 2 error (false negative- patient deemed not about to commit suicide, but in actuality is going to). So, instinctively, there is a leaning towards caution in these scenarios. After all, by the time you end up being evaluated at the hospital something probably needs to be done.1
II
The balancing of these two types of errors is one predicament. And it is article in of itself on whether it’s done well in the current healthcare world (I have doubts). But there is another force, beyond healthy caution, that pushes patients who are depressed into involuntary hospitalizations - lawsuits. For some reason, the US legal system has decided that doctors, especially psychiatrists, have a legal duty to predict the future. Namely, they should be able to reliably determine who will actually attempt suicide and who won’t. If you, as a doctor, discharge someone who goes on to take their life by suicide, you better have good documentation that you ‘did everything right’, good malpractice insurance if that fails, and good emotional grounding to handle the guilt and harsh words that are about to come from their family2. After all, you are the doctor who assessed them for risk, right?
This is the problem though - risk assessments are shoddy. Even if you accurately stratify their risk, sometimes people with low risk proceed to make a suicide attempt. Conversely, more often than not, ‘high-risk’ patients don’t attempt suicide. It’s a numbers game, and it’s not even an accurate one. Perhaps, clinical decisions in psychiatry should not be based on risk assessment alone. Anecdotally, one psychiatrist told me he has only had one patient that he evaluated and discharged who proceeded to immediately take their life by suicide. That patient was deemed ‘low risk’ and just straight up lied in the assessment. It’s hard to predict the future when you can’t even trust the information you are given to predict it.
As long a doctor feels the specter of a lawsuit hovering around - even a lawsuit brought about by actions that are outside of their control- they will act to keep that lawsuit at bay. This means there are many patients who, while in tremendous psychological distress, get involuntarily committed when they maybe did not need to. Maybe extra support and close follow-up are all they needed. Maybe they will feel violated that they came for help and are being held against their will at the hospital when they just want to go to their job in the morning so they aren’t at risk of losing their job which would cause more stress. Maybe they won’t trust reaching out for help again in the future? Maybe we are holding up some of the limited hospital beds from others with more intense, acute psychiatric qualms who would benefit tremendously from the inpatient stay. Maybe their insurance won’t cover the involuntary care, and they get handed a ridiculous 5 digit bill. It doesn’t matter - medicolegal incentives encourage hospitalization. And once hospitalized, these same forces discourage discharge. 3
The four pillars of medical ethics are (1) Beneficence, (2) non-maleficence, (3) autonomy, and (4) justice. In easier terms, (1) do good, (2) don’t do bad, (3) people get make their own decisions (even if you think they are bad ones), and (4) be fair. Balancing all of these when it comes to risk assessment and suicide is an impossible fiasco. And we, unfortunately, have a healthcare system that expects clinicians to solve this fiasco multiple times a day via relatively short encounters. Good-intentioned people do a poor job at things when the incentives are misaligned. It seems to me, that the legal system expecting clinicians to be clairvoyant4 is creating an incentive misalignment. That said, I can see why we ending up in this position because accountability in healthcare is not irrelevant, but I don’t see an easy solution.
At first, it may seem cruel not to admit everyone who is suspected of being suicidal. But it turns out, that is a lot of people. Society hasn’t set up the resources for that. Also, inpatient hospitalizations, despite their wrap-around support, very close monitoring, lots of support staff, are emotionally kind of ‘sterile’. If you are not literally going to kill yourself, there are (ideally) plenty of less intensive options where you don’t have to write with crayons (pencils can be weapons) and share a bedroom with acutely psychotic strangers. It’s not uncommon for someone to end up at an inpatient psychiatric unit because of their depressed mood and suicidal thoughts only to realize that they are not that suicidal and would much rather be at home.
Their harsh words are understandable; they just lost a loved one and feel that someone is at fault. Anyone who loses a loved one, and feels there is someone to blame, is going to have a lot to say.
Some people know the system works this way and game the system for secondary gain. The shelter, food, and support found at psychiatric hospitals are pretty nice looking if you are homeless, hungry, and emotionally exhausted. Tell the doctor the right magic words, and it’s very hard for them not to send you to a psychiatric hospital under fear of losing their license. It’s every psychiatrist’s nightmare to be in court and have the judge say ‘So he told you he was having thoughts of suicide and you sent him home?’.
Of course, it’s nice to provide solace to people in these situations. But I’d much rather provide solace in the form of free housing and food that doesn’t require covering the salaries of multiple doctors and healthcare staff, ancillary administration staff, malpractice insurances, laboratory workup, unnecessary medications, excessive documentation, etc. That would be a lot cheaper, and more importantly, it would free up the already limited, scarce psychiatric beds available.
Other ways doctors are expected to predict the future: who will become addicted to a medication, how long does the patient have to live/should they get hospice care, etc. As in the case of suicide, economic and legal forces seem to unjustifiably influence these clinical decisions
This is great, looking forward to reading the rest of your posts